
Exhibit 99.1
Targeting Major Advances in Treatment of CNS Disorders November 11th , 2022 I Nasdaq: RLMD 1
Disclosures Certain statements contained in this presentation or in other documents of Relmada Therapeutics, Inc. (the “Company”), along with certain statements that may be made by management of the Company orally in presenting this material, may contain “forward - lookin g statements.” These statements can be identified by the fact that they do not relate strictly to historic or current facts. Th ey use words such as “estimate,” “expect,” “intend,” “believe,” “plan,” “anticipate,” “projected” and other words and terms of similar mea nin g in connection with any discussion of future operating or financial performance or condition. These statements are based upon the cu rrent beliefs and expectations of the Company’s management and are subject to significant risks and uncertainties. Statements regar din g future action, future performance and/or future results, those relating to the timing for completion, and results of, schedul ed or additional clinical trials and the FDA’s or other regulatory review and/or approval and commercial launch and sales results ( if any) of the Company’s formulations and products and regulatory filings related to the same may differ from those set forth in the for war d - looking statements. Peak sales and market size estimates have been determined on the basis of market research and comparable product analysis, but no assurances can be given that such sales levels will be achieved, if at all, or that such market size estimates will prove accurate. Because actual results are affected by these and other potential risks, contingencies and uncertainties, the Company cautions investors that actual results may differ materially from those expressed or implied in any forward - looking statement. It is not possible to predict or identify all such risks, contingencies and uncertainties. The Company identifies some of these factors in its S ecu rities and Exchange Commission (“SEC”) filings on Forms 10 - K, 10 - Q and 8 - K, and investors are advised to consult the Company’s filings for a more complete listing of risk factors, contingencies and uncertainties affecting the Company and its business and finan cia l performance. The Company assumes no obligation to update forward - looking statements as circumstances change. Investors are advised to consult further disclosures that the Company makes or has made on related subjects in the Company’s Form 10 - K, 10 - Q and 8 - K reports. 2

Investment Highlights Highly Compelling Opportunity in REL - 1017 Multiple Catalysts Expected Over the Next 12 Months CNS Focus with Lead Program in Major Depressive Disorder (MDD) CNS= Central Nervous System **Our fiscal year end is December 31. The periods referred to in this slide are calendar years and quarters. 3
Major Depressive Disorder & REL - 1017
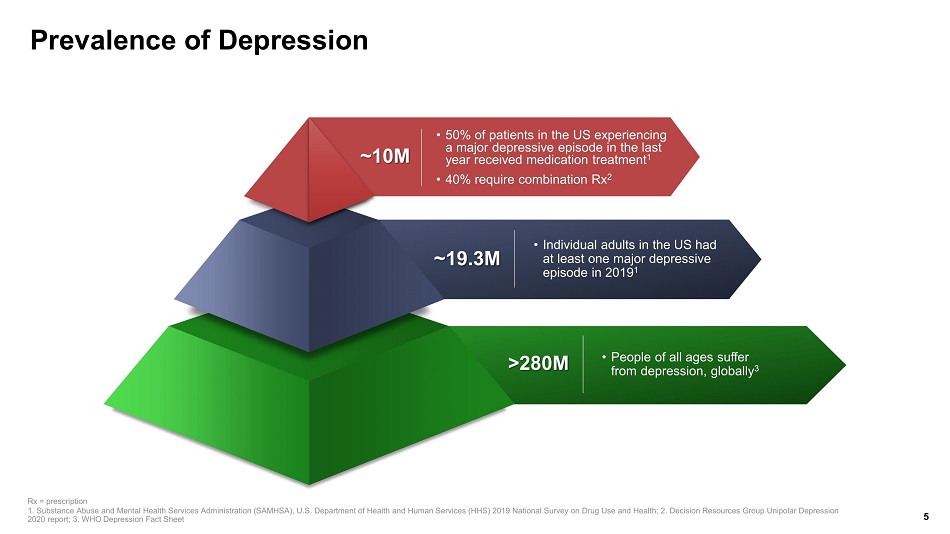
Prevalence of Depression ~10M • 50% of patients in the US experiencing a major depressive episode in the last year received medication treatment 1 • 40% require combination Rx 2 ~19.3M • Individual adults in the US had at least one major depressive episode in 2019 1 >280M • People of all ages suffer from depression, globally 3 5 Rx = prescription 1. Substance Abuse and Mental Health Services Administration (SAMHSA), U.S. Department of Health and Human Services (HHS) 201 9 N ational Survey on Drug Use and Health; 2. Decision Resources Group Unipolar Depression 2020 report; 3. WHO Depression Fact Sheet
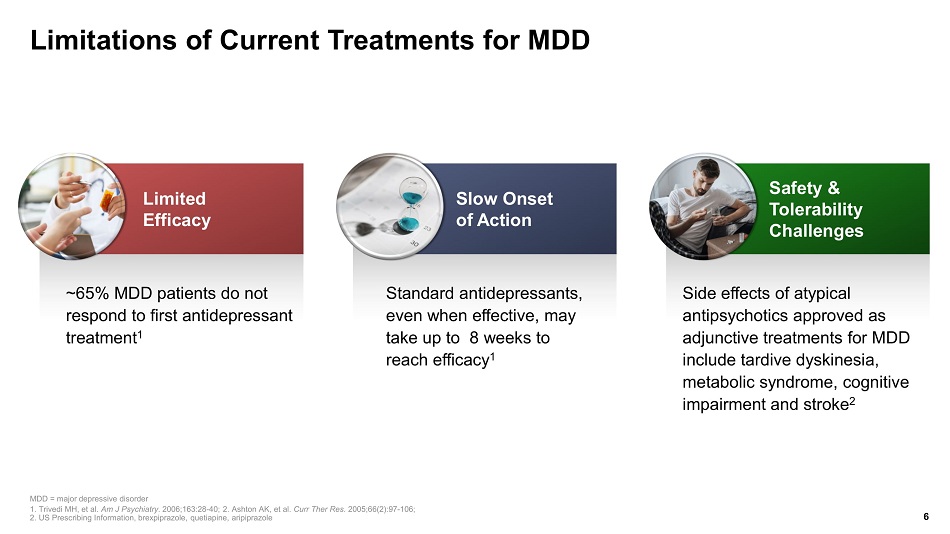
Limitations of Current Treatments for MDD ~65% MDD patients do not respond to first antidepressant treatment 1 Standard antidepressants, even when effective, may take up to 8 weeks to reach efficacy 1 MDD = major depressive disorder 1. Trivedi MH, et al. Am J Psychiatry. 2006;163:28 - 40; 2. Ashton AK, et al. Curr Ther Res. 2005;66(2):97 - 106; 2. US Prescribing Information, brexpiprazole , quetiapine, aripiprazole 6 Slow Onset of Action Side effects of atypical antipsychotics approved as adjunctive treatments for MDD include tardive dyskinesia, metabolic syndrome, cognitive impairment and stroke 2 Safety & Tolerability Challenges Limited Efficacy
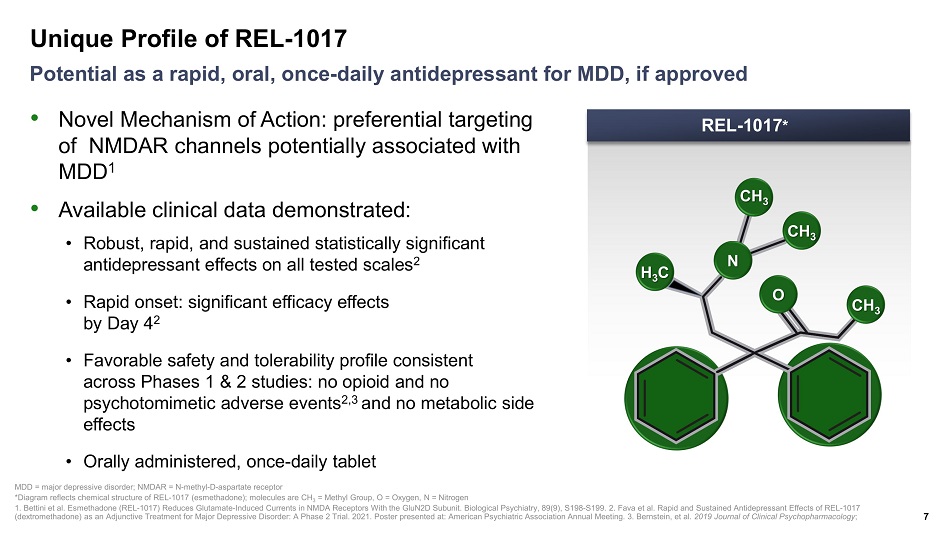
Unique Profile of REL - 1017 7 Potential as a rapid, oral, once - daily antidepressant for MDD, if approved MDD = major depressive disorder; NMDAR = N - methyl - D - aspartate receptor *Diagram reflects chemical structure of REL - 1017 ( esmethadone ); molecules are CH 3 = Methyl Group, O = Oxygen, N = Nitrogen 1. Bettini et al. Esmethadone (REL - 1017) Reduces Glutamate - Induced Currents in NMDA Receptors With the GluN2D Subunit. Biologica l Psychiatry, 89(9), S198 - S199. 2. Fava et al. Rapid and Sustained Antidepressant Effects of REL - 1017 ( dextromethadone ) as an Adjunctive Treatment for Major Depressive Disorder: A Phase 2 Trial. 2021. Poster presented at: American Psychiatric Ass ociation Annual Meeting. 3. Bernstein, et al. 2019 Journal of Clinical Psychopharmacology ; REL - 1017 * CH 3 CH 3 CH 3 O N H 3 C • Novel Mechanism of Action: preferential targeting of NMDAR channels potentially associated with MDD 1 • Available clinical data demonstrated: • Robust, rapid, and sustained statistically significant antidepressant effects on all tested scales 2 • Rapid onset: significant efficacy effects by Day 4 2 • Favorable safety and tolerability profile consistent across Phases 1 & 2 studies: no opioid and no psychotomimetic adverse events 2,3 and no metabolic side effects • Orally administered, once - daily tablet

REL - 1017 Ph 1 & 2 Efficacy & Safety Data
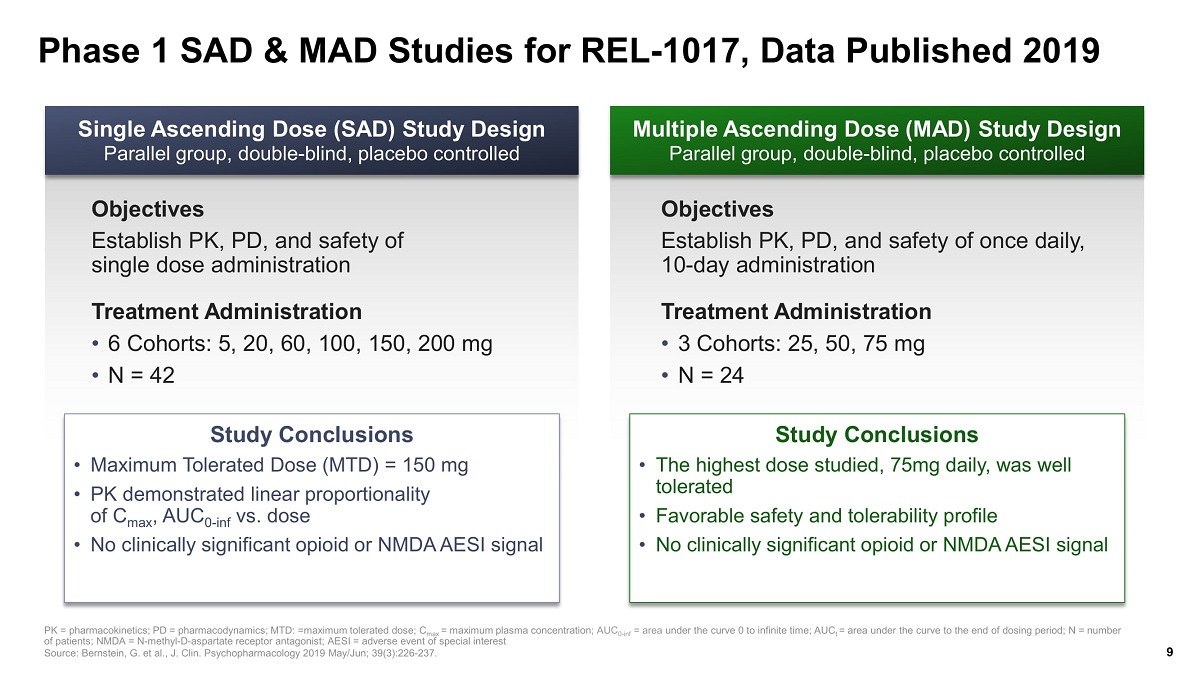
Phase 1 SAD & MAD Studies for REL - 1017, Data Published 2019 PK = pharmacokinetics; PD = pharmacodynamics; MTD: =maximum tolerated dose; C max = maximum plasma concentration ; AUC 0 - inf = area under the curve 0 to infinite time; AUC t = area under the curve to the end of dosing period; N = number of patients; NMDA = N - methyl - D - aspartate receptor antagonist; AESI = adverse event of special interest Source: Bernstein, G. et al., J. Clin. Psychopharmacology 2019 May/Jun; 39(3):226 - 237. Multiple Ascending Dose (MAD) Study Design Parallel group, double - blind, placebo controlled Single Ascending Dose (SAD) Study Design Parallel group, double - blind, placebo controlled Objectives Establish PK, PD, and safety of single dose administration Treatment Administration • 6 Cohorts: 5, 20, 60, 100, 150, 200 mg • N = 42 Objectives Establish PK, PD, and safety of once daily, 10 - day administration Treatment Administration • 3 Cohorts: 25, 50, 75 mg • N = 24 Study Conclusions • Maximum Tolerated Dose (MTD) = 150 mg • PK demonstrated linear proportionality of C max , AUC 0 - inf vs. dose • No clinically significant opioid or NMDA AESI signal Study Conclusions • The highest dose studied, 75mg daily, was well tolerated • Favorable safety and tolerability profile • No clinically significant opioid or NMDA AESI signal 9
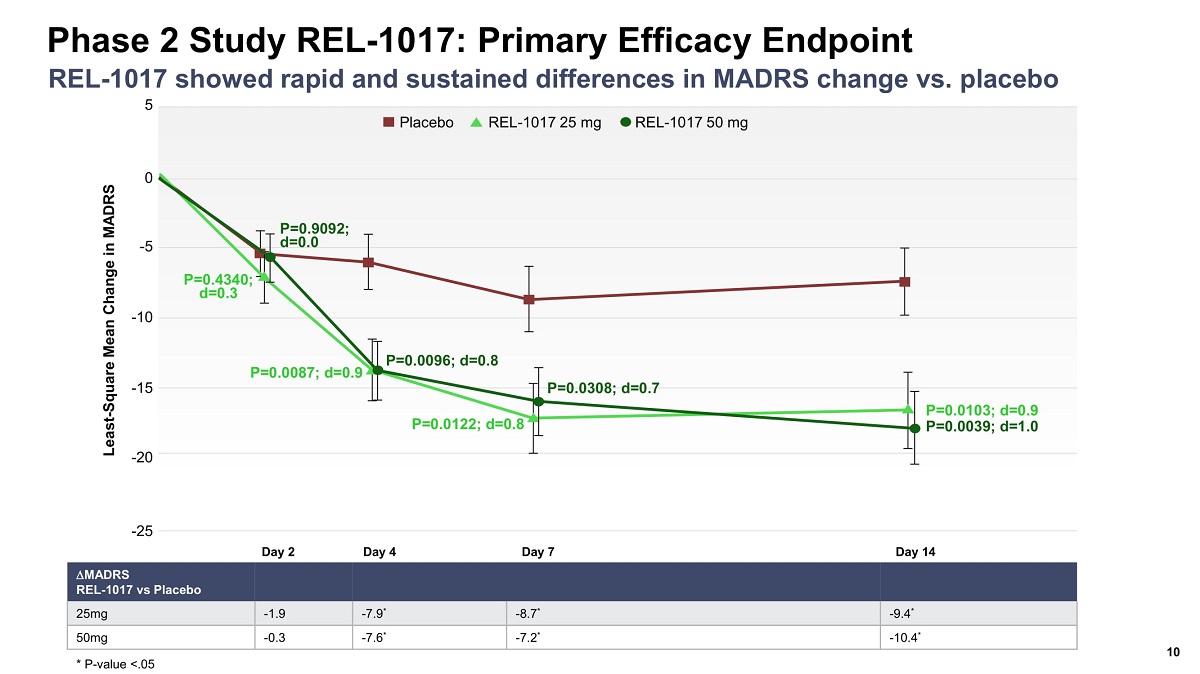
Phase 2 Study REL - 1017: Primary Efficacy Endpoint 10 REL - 1017 showed rapid and sustained differences in MADRS change vs. placebo Day 2 Day 4 Day 7 Day 14 5 0 - 5 - 25 Least - Square Mean Change in MADRS - 10 - 15 - 20 P=0.0103; d=0.9 P=0.0039; d=1.0 P=0.0308; d=0.7 P=0.0122; d=0.8 P=0.0096; d=0.8 P=0.0087; d=0.9 P=0.9092; d=0.0 P=0.4340; d=0.3 Placebo REL - 1017 25 mg REL - 1017 50 mg MADRS REL - 1017 vs Placebo 25mg - 1.9 - 7.9 * - 8.7 * - 9.4 * 50mg - 0.3 - 7.6 * - 7.2 * - 10.4 * * P - value <.05
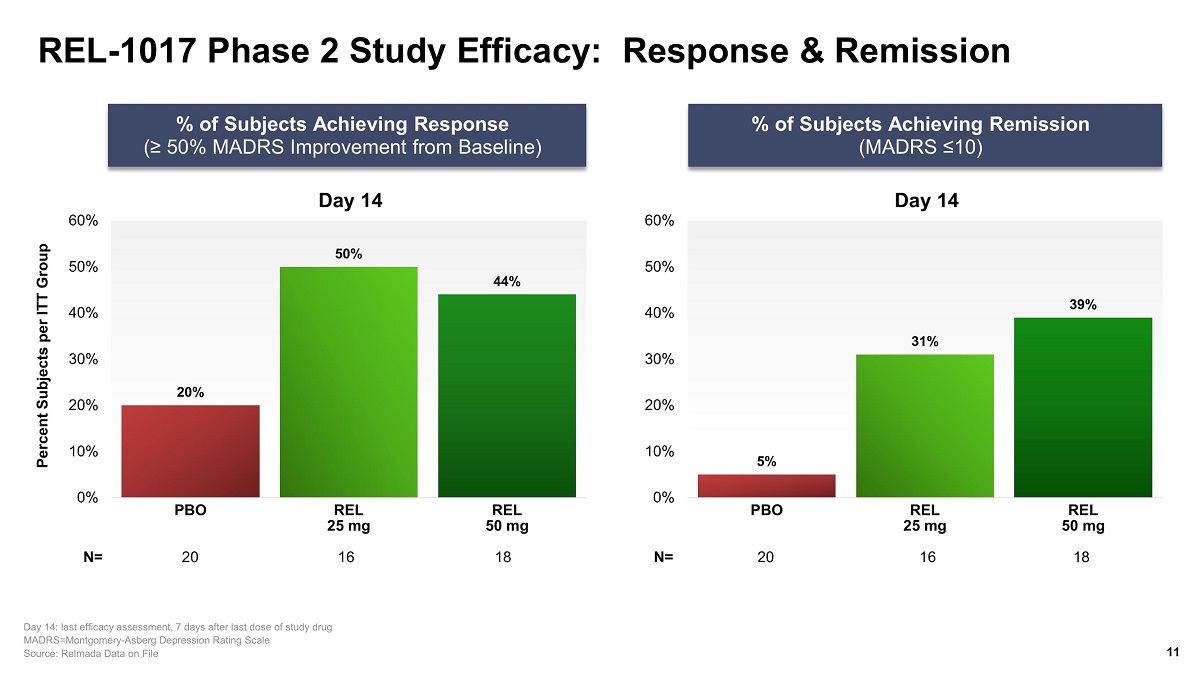
REL - 1017 Phase 2 Study Efficacy: Response & Remission % of Subjects Achieving Remission (MADRS ≤10) Percent Subjects per ITT Group % of Subjects Achieving Response (≥ 50% MADRS Improvement from Baseline) 11 Day 14: last efficacy assessment, 7 days after last dose of study drug MADRS=Montgomery - Asberg Depression Rating Scale Source: Relmada Data on File N= Day 14 20% 50% 44% 0% 10% 20% 30% 40% 50% 60% PBO REL 25 mg REL 50 mg 20 16 18 Day 14 5% 31% 39% 0% 10% 20% 30% 40% 50% 60% PBO REL 25 mg REL 50 mg 20 16 18 N=
Safety & Tolerability Findings from Phase 2 • Only Mild and Moderate transient AEs – no SAEs • No increased prevalence of specifically relevant organ group AEs in treatment groups vs placebo • No evidence of opiate effects or withdrawal symptoms in treatment groups vs placebo • No evidence of treatment - induced dissociative or psychotomimetic symptoms in the treatment groups vs placebo 12 Safety & Tolerability Comparable to Placebo AE = adverse event; SAE = serious adverse event Source: Fava et al. Rapid and Sustained Antidepressant Effects of REL - 1017 ( dextromethadone ) as an Adjunctive Treatment for Major Depressive Disorder: A Phase 2 Trial. 2021. Poster presented at: American Psychiatric Ass ociation Annual Meeting
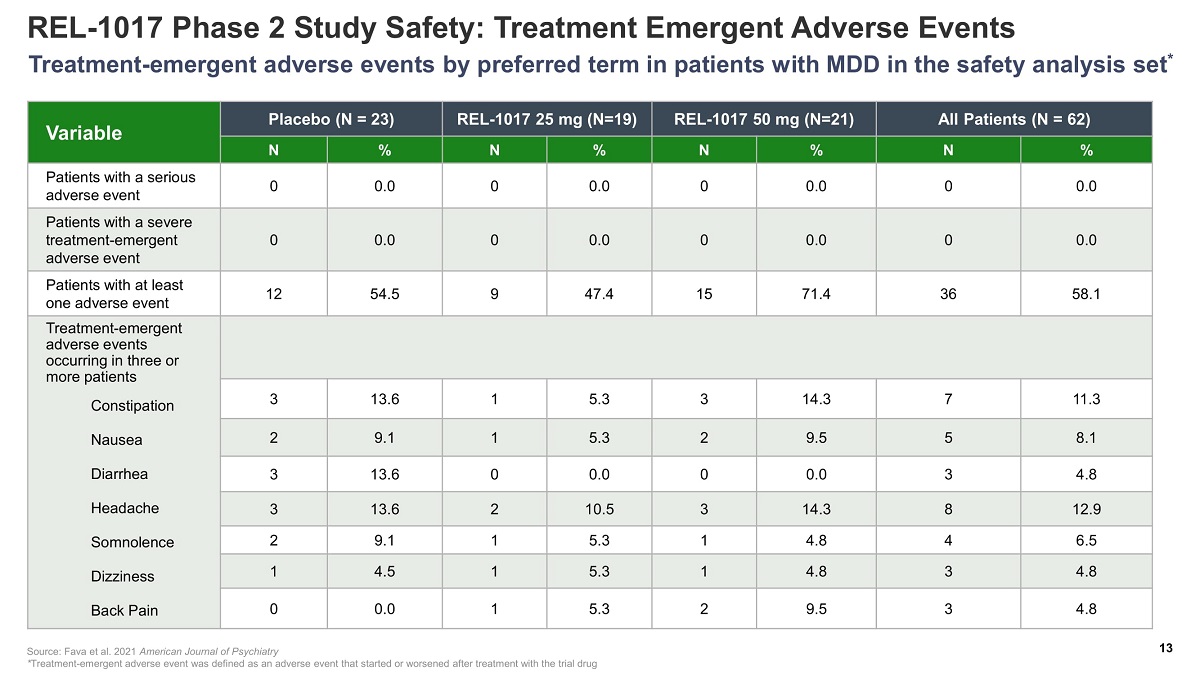
REL - 1017 Phase 2 Study Safety: Treatment Emergent Adverse Events Variable Placebo (N = 23) REL - 1017 25 mg (N=19) REL - 1017 50 mg (N=21) All Patients (N = 62) N % N % N % N % Patients with a serious adverse event 0 0.0 0 0.0 0 0.0 0 0.0 Patients with a severe treatment - emergent adverse event 0 0.0 0 0.0 0 0.0 0 0.0 Patients with at least one adverse event 12 54.5 9 47.4 15 71.4 36 58.1 Treatment - emergent adverse events occurring in three or more patients Constipation Nausea Diarrhea Headache Somnolence Dizziness Back Pain 3 13.6 1 5.3 3 14.3 7 11.3 2 9.1 1 5.3 2 9.5 5 8.1 3 13.6 0 0.0 0 0.0 3 4.8 3 13.6 2 10.5 3 14.3 8 12.9 2 9.1 1 5.3 1 4.8 4 6.5 1 4.5 1 5.3 1 4.8 3 4.8 0 0.0 1 5.3 2 9.5 3 4.8 Treatment - emergent adverse events by preferred term in patients with MDD in the safety analysis set * Source: Fava et al. 2021 American Journal of Psychiatry * Treatment - emergent adverse event was defined as an adverse event that started or worsened after treatment with the trial drug 13
14 The results of experimental studies predictive of human abuse potential 1 and the results of human abuse potential studies in recreational opioid users 2 and in recreational ketamine users 3 indicate no meaningful abuse potential and support the DEA statement below: “The d - isomer lacks significant respiratory depressant action and addiction liability...” US Drug Enforcement Administration December 2019 4 1. Henningfield , J., Gauvin, D., Bifari , F. et al. REL - 1017 ( esmethadone ; D - methadone) does not cause reinforcing effect, physical dependence and withdrawal signs in Sprague Dawley rats. Sci Rep 12, 1 1389 (2022) 2. Shram M, Henningfield J, Apseloff G, Gorodetzky C, De Martin S, Vocci F, Sapienza F, Kosten T, Huston J, Buchhalter A, Ashworth J, Lanier R, Folli F, Traversa S, Inturrisi CE, Manfredi P, & Pappagallo M. No meaningful abuse potential in recreational opioid users of REL - 1017 ( esmethadone hydrochloride), a new NMDAR antagonist and potential rapid - acting antidepressant American Society of Clinical Psychopharmacolog y (ASCP) 2022 3. Shram M, Henningfield J, Apseloff G, Gorodetzky C, De Martin S, Vocci F, Sapienza F, Kosten T, Huston J, Buchhalter A, Ashworth J, Lanier R, Folli F, Traversa S, Inturrisi CE, Manfredi P, & Pappagallo M. No meaningful abuse potential in recreational ketamine users of REL - 1017 ( esmethadone hydrochloride), a new NMDAR antagonist and potential rapid - acting antidepressant. American Society of Clinical Psychopharmacolo gy (ASCP) 2022 4. US DEA Statement on Methadone, December 2019 https:// www.deadiversion.usdoj.gov / drug_chem_info /methadone/ methadone.pdf#search =methadone last access February 2022
Reliance: The Phase 3 Program for REL - 1017
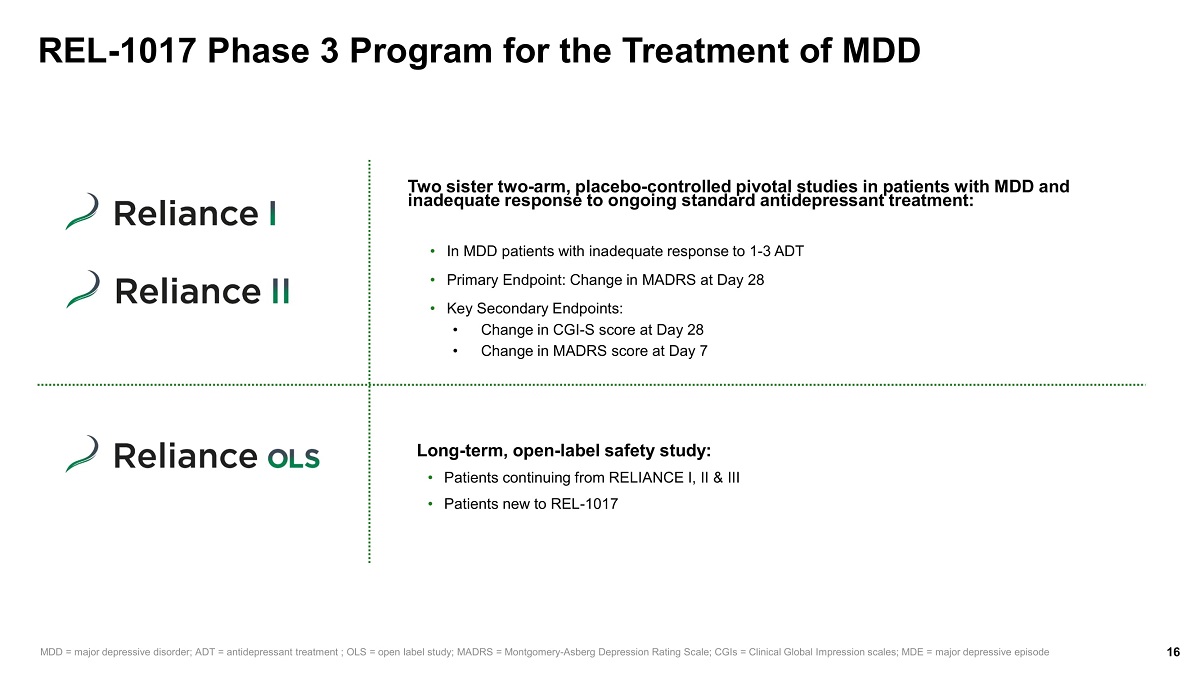
REL - 1017 Phase 3 Program for the Treatment of MDD 16 Two sister two - arm, placebo - controlled pivotal studies in patients with MDD and inadequate response to ongoing standard antidepressant treatment: • In MDD patients with inadequate response to 1 - 3 ADT • Primary Endpoint: Change in MADRS at Day 28 • Key Secondary Endpoints: • Change in CGI - S score at Day 28 • Change in MADRS score at Day 7 MDD = major depressive disorder; ADT = antidepressant treatment ; OLS = open label study; MADRS = Montgomery - Asberg Depression Rating Scale; CGIs = Clinical Global Impression scales; MDE = major depressive episode Long - term, open - label safety study: • Patients continuing from RELIANCE I, II & III • Patients new to REL - 1017
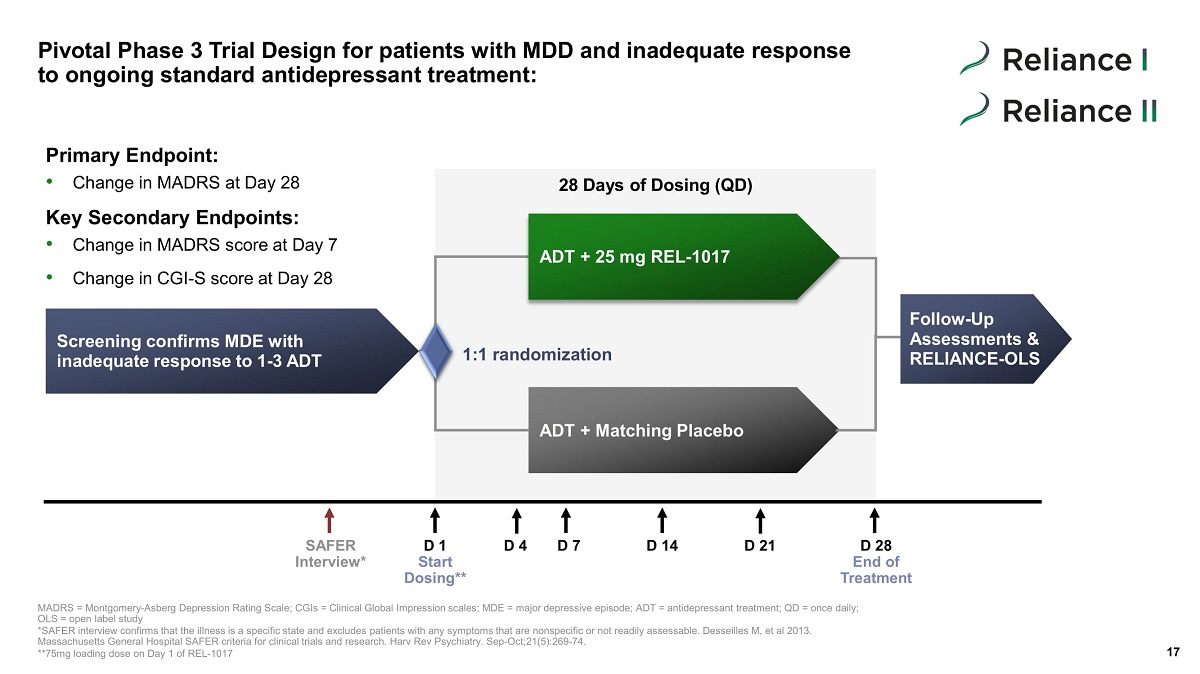
Screening confirms MDE with inadequate response to 1 - 3 ADT ADT + 25 mg REL - 1017 ADT + Matching Placebo Pivotal Phase 3 Trial Design for patients with MDD and inadequate response to ongoing standard antidepressant treatment: 17 1:1 randomization 28 Days of Dosing (QD) Follow - Up Assessments & RELIANCE - OLS SAFER Interview* D 1 Start Dosing** D 4 D 7 D 14 D 28 End of Treatment D 21 MADRS = Montgomery - Asberg Depression Rating Scale; CGIs = Clinical Global Impression scales; MDE = major depressive episode; ADT = antidepressant treat me nt; QD = once daily; OLS = open label study *SAFER interview confirms that the illness is a specific state and excludes patients with any symptoms that are nonspecific o r n ot readily assessable. Desseilles M, et al 2013. Massachusetts General Hospital SAFER criteria for clinical trials and research. Harv Rev Psychiatry. Sep - Oct;21(5):269 - 74. **75mg loading dose on Day 1 of REL - 1017 Primary Endpoint: • Change in MADRS at Day 28 Key Secondary Endpoints: • Change in MADRS score at Day 7 • Change in CGI - S score at Day 28
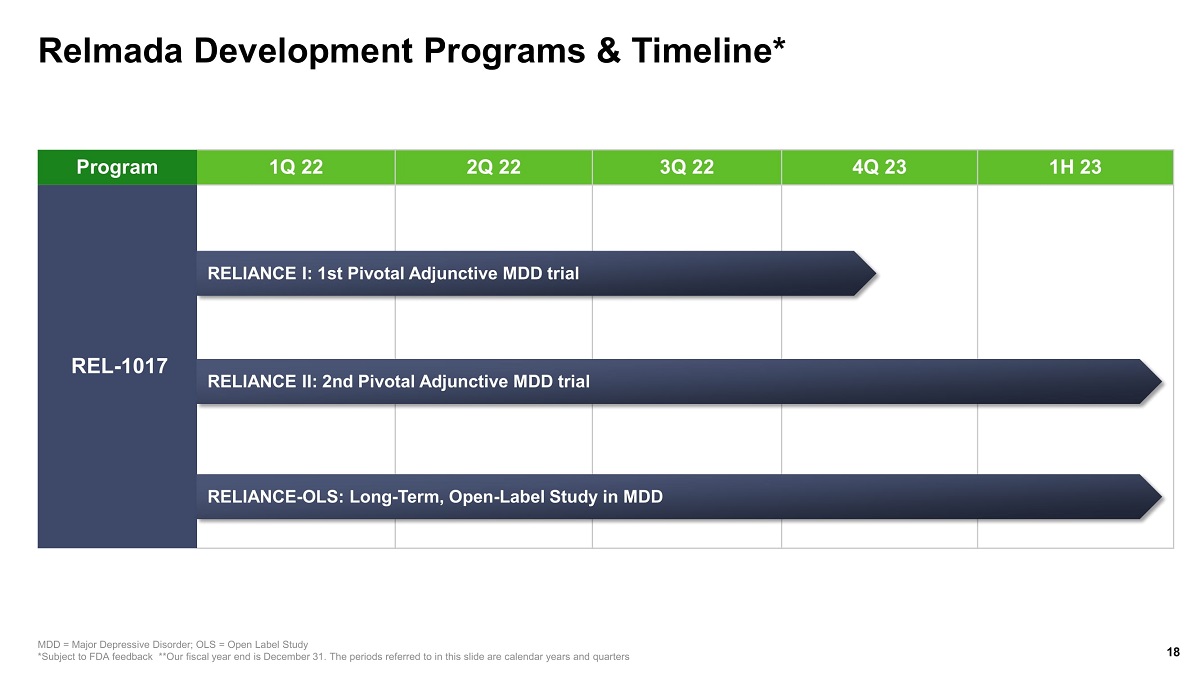
Relmada Development Programs & Timeline* 18 MDD = Major Depressive Disorder; OLS = Open Label Study *Subject to FDA feedback **Our fiscal year end is December 31. The periods referred to in this slide are calendar years and qua rters Program 1Q 22 2Q 22 3Q 22 4Q 23 1H 23 REL - 1017 RELIANCE I: 1st Pivotal Adjunctive MDD trial RELIANCE II: 2nd Pivotal Adjunctive MDD trial RELIANCE - OLS: Long - Term, Open - Label Study in MDD
Neuroplastogen TM Program
We have a pipeline of molecules with neural plasticity modulating activity for the treatment of CNS disorders 20 We are developing a novel psilocybin formulation and we are synthetizing psilocybin derivatives with promising therapeutic activity We have synthesized a series of novel esmethadone derivatives with NMDAR regulating activity. We are in the process of selecting the most promising candidates for advancing their development in the treatment of CNS disorders Novel esmethadone derivatives Novel psilocybin formulation and novel psilocybin derivatives CNS = Central Nervous System; NMDAR = N - methyl - D - aspartate receptor

Corporate Information
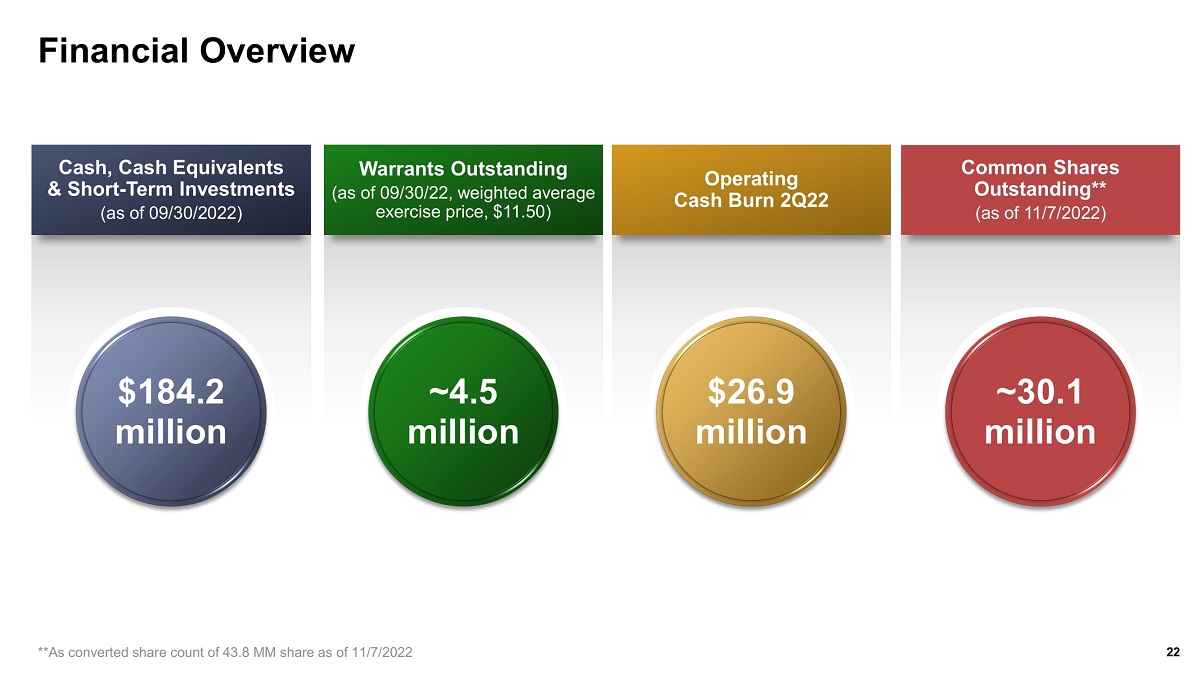
Financial Overview Cash, Cash Equivalents & Short - Term Investments (as of 09/30/2022) $184.2 million Warrants Outstanding (as of 09/30/22, weighted average exercise price, $11.50) ~4.5 million Operating Cash Burn 2Q22 $26.9 million Common Shares Outstanding** (as of 11/7/2022) ~30.1 million 22 **As converted share count of 43.8 MM share as of 11/7/2022
Investment Highlights Highly Compelling Lead Product Opportunity in REL - 1017 Key Catalysts Expected Over the Next 12 Months Focus on CNS diseases and Lead Program in Major Depressive Disorder (MDD) CNS= Central Nervous System;; MDD = major depressive disorder; MOA = mechanism of action **Our fiscal year end is December 31. The periods referred to in this slide are calendar years and quarters. 1. WHO Depression Fact Sheet; 2. Al - Harbi K.S. 2012 Patient Preference and Adherence; 3. . Fava et al. Rapid and Sustained Antidepressant Effects of REL - 1017 ( dextromethadone ) as an Adjunctive Treatment for Major Depressive Disorder: A Phase 2 Trial. 2021. Poster presented at: American Psychiatric Association Annual Meeting 23 • Novel MOA with successful Phase 2 trial in adjunctive MDD that showed statistically significant, robust, rapid, and sustained antidepressant effects with favorable safety and tolerability profile 3 • Phase 3 program underway following successful end of Phase 2 Meeting with the FDA • Strong intellectual property position around REL - 1017 with expirations through the mid/late - 2030s • REL - 1017, l ead candidate, is in Phase 3 for depression, a leading cause of disability worldwide 1 • CNS focus, with expertise in developing novel therapeutics that show potential for neuroplasticity • 50% – 66% of patients with depression do not fully recover on an antidepressant medication 2 • Standard antidepressants can take 2 - 8 weeks to work and have significant side - effects • Completion of RELIANCE I adjunctive MDD trial expected 4Q 2022 • Completion of RELIANCE II adjunctive MDD trial expected in 2023 • Completion of RELIANCE – OLS (Long - term, Open - label study in MDD) expected in 1H 2023